Male Infertility & Varicocele
What couples need to know when “the problem” may lie in the veins around the male organ.
1. Why focus on the male partner?
About 15% of couples struggle to conceive after a year of unprotected intercourse, and in roughly half of those cases a male factor is present. (uroweb.org)
Yet many evaluations (and internet searches!) still centre on the female partner; understanding common male contributors keeps couples from losing precious time.
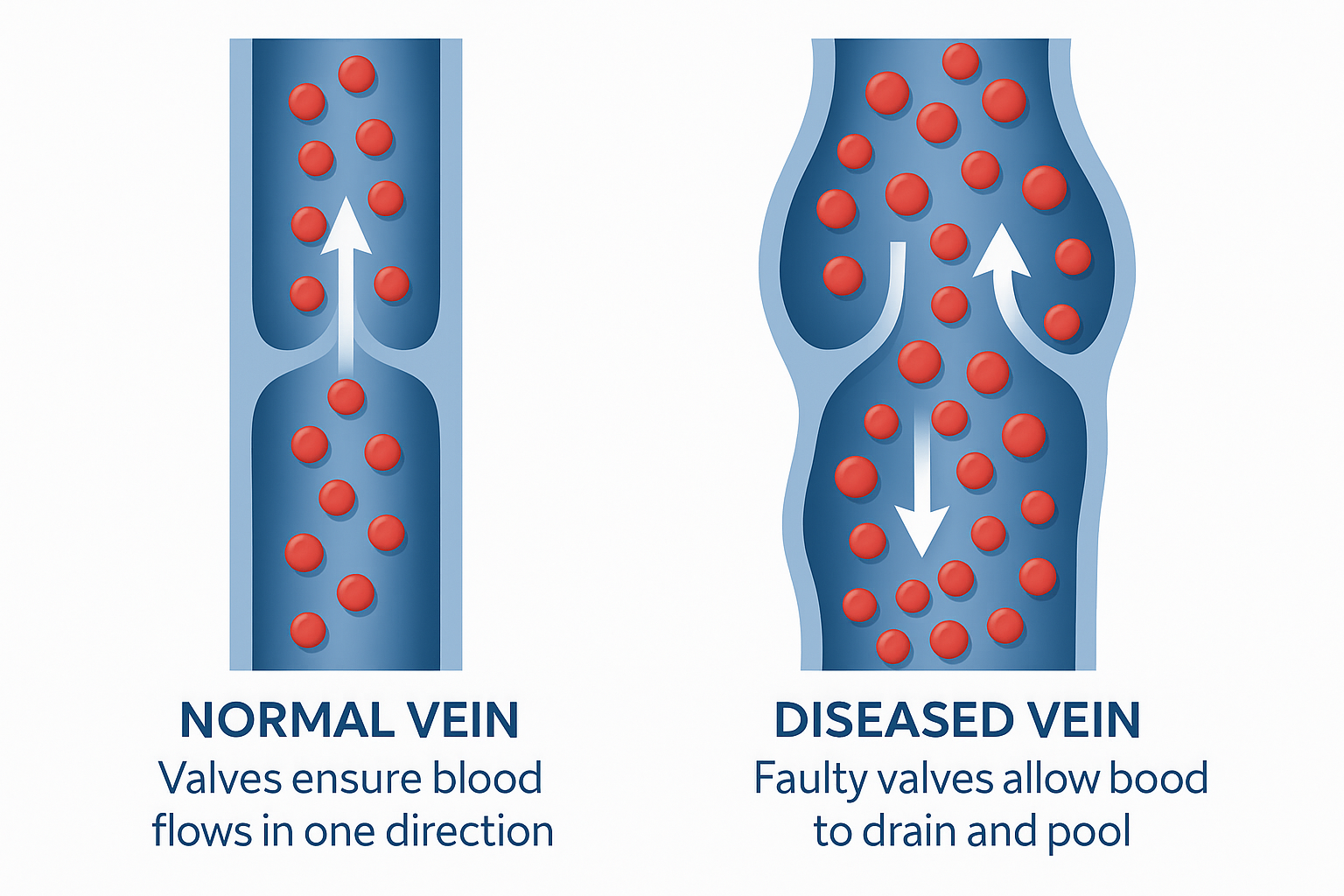
2. Varicocele 101
A varicocele is an enlargement of the pampiniform venous plexus—think “varicose veins of the scrotum.”
How common? 10–20% of all men, 35–40% of men with primary infertility, and up to 80% with secondary infertility.
Typical clues: a painless “bag-of-worms” feeling, dull scrotal ache that worsens standing or after exercise, or abnormal semen analysis found during an infertility work-up.
3. How can a varicocele hurt fertility?
Research points to several, often overlapping, mechanisms: increased scrotal temperature, low-grade testicular hypoxia, reflux of adrenal/renal metabolites and spikes in reactive oxygen species—all of which can disrupt sperm production, DNA integrity and even testosterone output.
4. Detecting the problem
Hands-on exam by an andrology-trained urologist remains the cornerstone.
Grading (I–III) is based on size/palpability.
Colour-Doppler ultrasound is reserved for equivocal cases or recurrences; sub-clinical (ultrasound-only) varicoceles do not merit routine repair under today’s guidelines.
5. When do guidelines suggest treatment?
International societies (AUA/ASRM, EAU, others) agree on three green lights for surgery:
| You have… | And… | Therefore… |
|---|---|---|
| A palpable varicocele | Abnormal semen parameters or symptomatic scrotal pain or testicular growth arrest (boys/teens) | Offer varicocelectomy |
| Sub-clinical varicocele | Normal semen | Do not operate |
| Couple planning IVF/ICSI soon | Time is critical | Discuss pros/cons; evidence of extra IVF benefit is limited |
(wjmh.org)
6. What is a varicocelectomy?
A procedure that interrupts or blocks the faulty veins, rerouting blood through healthy pathways. Main approaches:
| Approach | Typical incision/access | Recurrence | Hydrocele risk | Notes |
|---|---|---|---|---|
| Microsurgical sub-inguinal | 2-3 cm at groin root | ~2% | 2% | Gold standard; spares arteries & lymphatics |
| Microsurgical inguinal | Small groin incision | ~2–3% | 2% | Similar outcomes, slightly higher pain |
| Laparoscopic (mass-ligation) | 3 keyholes on abdomen | ~3% | Up to 11% | Quick, but higher hydrocele rate |
| Radiologic embolisation/sclerotherapy | Needle via vein in arm/leg | 7% | <1% | No cut; higher technical failure (≈10%) |
Figures derived from a 2023 systematic review of >4,000 cases. (pubmed.ncbi.nlm.nih.gov)
7. Does it actually improve fertility?
Semen quality: Meta-analysis within the 2024 EAU guideline update shows significant gains in sperm concentration, total count, motility and morphology after repair, especially in men who started with abnormal results. (uroweb.org)
Pregnancy & live-birth: A 2024 meta-analysis of seven RCTs reported a 4-fold higher chance of natural pregnancy after varicocelectomy (OR 4.15). (wjmh.org)
Translation: Roughly 1 in 4–5 couples who would otherwise need assisted reproduction conceive naturally after the man’s veins are fixed.
Pain relief: ~80% of men with dull scrotal ache report durable relief post-surgery.
8. Recovery at a glance
| Milestone | Typical timeline |
|---|---|
| Home the same day | ✔ |
| Light office work | 2–3 days |
| Gym / heavy lifting | 2–4 weeks |
| Semen re-test | 3 months (full effect may take 6–9 months) |
| Trying to conceive | Resume when comfortable; count the 3-, 6- and 9-month marks for improvements |
Minor bruising and swelling are common; serious issues such as hydrocele, infection or recurrence are uncommon (<3% in micro-surgery). (pubmed.ncbi.nlm.nih.gov)
9. Where does surgery fit with IVF/ICSI?
Before ART: Repair can raise natural pregnancy odds and improve sperm DNA fragmentation, which may translate to higher success and lower miscarriage rates with IVF/ICSI. (uroweb.org)
After repeated IVF failure: A male-factor reassessment (including hunting for an overlooked varicocele) is worthwhile.
10. Key take-aways
- Varicocele is the single most common, surgically correctable cause of male infertility.
- Modern microsurgical repair is quick, outpatient and boasts >95% success with <3% complications.
- Men with a palpable varicocele and abnormal semen—or bothersome pain—should talk to a urologist experienced in male reproduction.
- Expect tangible sperm improvements by 3–6 months and a meaningful bump in pregnancy odds within a year.
- Shared decision-making matters: weigh female age, existing ART plans and personal timelines.